



Visit our Re-post guidelines
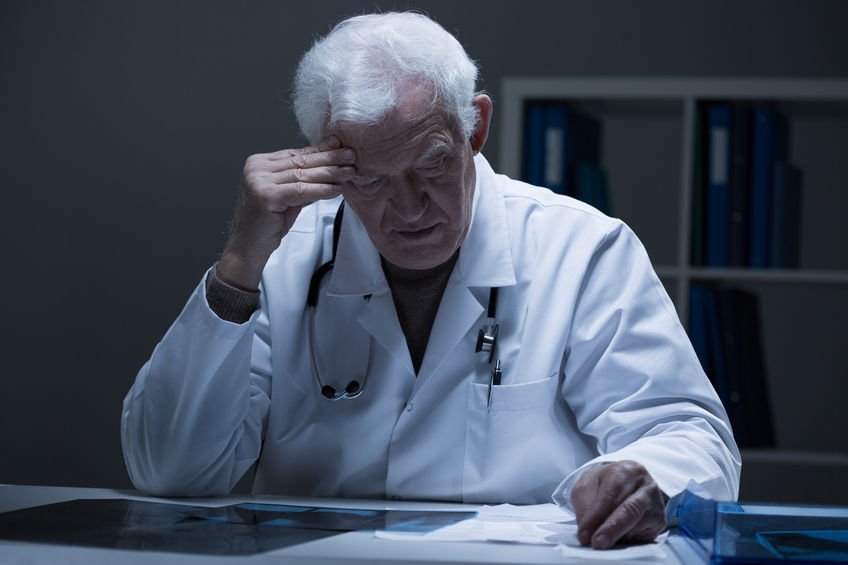
What if everything your doctor told you about osteoporosis and osteopenia was wrong?
What if osteoporosis were not the primary cause of fractures in aging populations? What if both the definitions of osteoporosis and osteopeniaused to justify pharmaceutical treatment were both misleading and age inappropriate?
These are questions we explored in a previous exposé titled, “Osteoporosis Myth: The Dangers of High Bone Mineral Density,” wherein we explored evidence showing the so-called “osteoporosis epidemic” is not an evidence-based concept but a manufactured one designed to serve the interests of a growing industrial medical/pharmaceutical complex.
A paper published in the Journal of Internal Medicine titled, “Osteoporosis: the emperor has no clothes,” confirms that the primary cause of what are normally labeled “osteoporotic fractures” are falls and related modifiable lifestyle factors and not osteoporosis, i.e. abnormally “porous” or low-density bones.
The new study pointed out three false notions that can be disputed:
-
Mistaken pathophysiology: “Most fracture patients have fallen, but actually do not have osteoporosis. A high likelihood of falling, in turn, is attributable to an ageing-related decline in physical functioning and general frailty.”
-
Ineffective screening: “Currently available fracture risk prediction strategies including bone densitometry and multifactorial prediction tools are unable to identify a large proportion of patients who will sustain a fracture, whereas many of those with a high fracture risk score will not sustain a fracture.”
-
Unproven and unsafe treatment: “The evidence for the viability of bone-targeted pharmacotherapy in preventing hip fracture and other clinical fragility fractures is mainly limited to women aged 65–80 years with osteoporosis, whereas the proof of hip fracture-preventing efficacy in women over 80 years of age and in men at all ages is meagre or absent. Further, the antihip fracture efficacy shown in clinical trials is absent in real-life studies. Many drugs for the treatment of osteoporosis have also been associated with increased risks of serious adverse events. There are also considerable uncertainties related to the efficacy of drug therapy in preventing clinical vertebral fractures, whereas the efficacy for preventing other fractures (relative risk reductions of 20–25%) remains moderate, particularly in terms of the low absolute risk reduction in fractures with this treatment”
The open access study is well worth reading in its entirety, but below are a few takeaways that we want to highlight.
Falling and Not Low Bone Mineral Density Is The Primary Cause of Fractures
Millions of men and women whose bones are actually normal for their age group (Z-score) are being manipulated into thinking that their bones should remain as dense as an approximately 30-year-old young adult (T-score) despite the natural process of bone thinning and reduction of density that attends the aging process. This T-score based bone density system pathologizes/over-medicalizes normal bone density variations, creating disease diagnoses where none should be found — a situation that is incredibly lucrative from the perspective of the bottom line of pharmaceutical and medical services companies. This has lead to a massive problem with overdiagnosis and overtreatment — two euphemistic technical terms to describe what happens when asymptomatic and otherwise healthy populations are told they have a ‘specific disease’ that they do not have (overdiagnosis), and subsequently pressured into taking pharmaceuticals (overtreatment), whose adverse effects often contribute to morbidity and premature mortality.
The reality, however, is that falling and not low bone mineral density are the primary reason why fractures occur. Since it is a statistical fact that the older you get the more often you fall, and since the older you get the less dense your bones become, it is easy to confuse the lower bone mineral density as a “cause” and not just an “association” with increased fracture risk. The authors of the new study provided this clever cartoon to drive the point home:
.png)
Given the reality behind what causes (and prevents) fracture, exercise and its resultant muscular and neurological health effects are of vital importance when it comes to minimizing the risk of falls, as well as surviving them without a fracture. And yet the reality is that the x-ray based DXA scans used to ascertain bone density do nothing but determine the density of the skeletal system, and not bone quality, i.e. strength. Nor can the DXA scan ascertain the structure/function (and therefore health) of the other tissues within the body that directly contribute to determining the risk of falling and the effects that the impact of a fall will have on the skeletal system. The following diagram shows the discrepancy that emerges between reality and the DXA image:

Where is the Evidence for Pharmaceutical “Prevention” of Fracture?
While anti-resportive bone drugs like Fosamax (a bisphosphonate) may contribute to increased bone mineral density, they do not necessarily improve bone quality and strength. Very dense bone created by destroying osteoclasts (bone-degrading cells) may be far more brittle than less dense bone where there is healthy turnover of the osteoclasts and osteoblasts (bone-building cells). In fact, drugs like Fosamax are notorious for contributing to bone degeneration in the jawbone (osteonecrosis). Also, we have discovered an extensive body of research indicating higher-than-normal bone density greatly increases the risk of malignant breast cancer, further calling into question the present day fixation on increasing bone density at any cost with highly toxic calcium supplements and drugs. Moreover, the new study points out that meta-analyses of the clinical literature on pharmacological treatment of osteoporosis for fracture risk reduction have produced almost no supportive evidence. Despite this, they point out that, “Osteoporosis guidelines systematically ignore the obvious ‘evidence void’ in the RCTs.”

The authors conclude: “Given all this, should ‘osteoporosis’ be added to a long list of diagnoses for which doing less, or even nothing, is better than our contemporary practice?”
Thankfully, we don’t just have to “do nothing.” Exercise, nutrition, and practices like yoga, tai chi, etc., can go a long way to reduce the risk of fracture, as well as supporting healthy bone mineral density, and more importantly, bone strength and structural integrity. To learn more use our natural osteoporosis prevention and treatment database to explore study abstracts and articles relevant to this topic.
Originally published: 2017-06-29 Article updated: 2019-10-30

![]()
Come Follow Us on Twitter
Come Like Us on Facebook
Check us out on Instagram
And Sign Up for our Newsletter